As October is Breast Cancer Awareness Month, now is a great time to clear up questions and misconceptions that many women, including my patients over the years, have had when considering a mammogram. Hopefully by sharing the facts I can offer you a level of comfort and understanding of the mammography experience.
 Elizabeth Wende Breast Care (EWBC), where I am an attending radiologist, recommends that average-risk women begin screening mammograms at age 40 and every year thereafter for as long as they are reasonably healthy. Also, we have found that women with a strong family history of breast cancer benefit from earlier screenings and should consult their physician about when to start mammography and if additional imaging, such as an MRI, is required.
Elizabeth Wende Breast Care (EWBC), where I am an attending radiologist, recommends that average-risk women begin screening mammograms at age 40 and every year thereafter for as long as they are reasonably healthy. Also, we have found that women with a strong family history of breast cancer benefit from earlier screenings and should consult their physician about when to start mammography and if additional imaging, such as an MRI, is required.
In addition, we believe women need to perform monthly breast exams and continue yearly check-ups and clinical breast exams by their health care providers. Some breast cancers, especially in women with dense breast tissue, may be found by breast exam in-between the time interval for screening mammography. It is important that breast exams continue to be performed. We disagree with the recent American Cancer Society recommendations to discontinue breast examinations.
Our recommendations are consistent with the American College of Radiology and Society of Breast Imaging, and are based on and supported by several long-term studies. Forty years of our own patient data also supports annual screening as a considerable number of the breast cancers that we diagnose through screening mammography is in our young patients ages 40-50. We believe early detection leads to lifesaving outcomes.
The Facts:
• The most important benefit of screening mammography is to find breast cancer EARLY, when the cancer is most treatable and survivable.
• Breast cancer is the number one cause of death in women ages 35-54.
• Mammography has been proven to reduce deaths due to breast cancer in women screened beginning at age 40.
• 25% of all years of life lost to breast cancer occur in women diagnosed before the age of 45.
• Women at “high risk” for breast cancer due to known or suspected disease-causing
mutation (such as BRCA1 or BRCA2 genes, along with several other genes more recently identified) should begin screening as early as 25 and include MRI.
• About 10 percent of women having
a screening mammogram will be called back (recalled) for extra testing or views.
 THIS IS NORMAL. Among women called back, 95 percent do not have cancer. Several studies surveying women after a call back (which turned out to be a false alarm) reveal that these women would and do come back yearly for mammography. In addition, the survey found the risks and side effects of a call back are exaggerated in both the media and some reports stating false alarms as a reason to skip mammography screening.
THIS IS NORMAL. Among women called back, 95 percent do not have cancer. Several studies surveying women after a call back (which turned out to be a false alarm) reveal that these women would and do come back yearly for mammography. In addition, the survey found the risks and side effects of a call back are exaggerated in both the media and some reports stating false alarms as a reason to skip mammography screening.
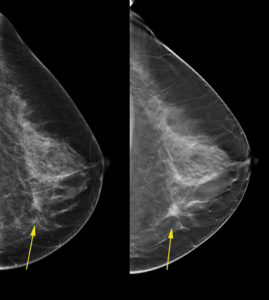
• New technologies, such as 3D mammography (also called digital breast tomosynthesis), are better able to identify cancer and can reduce call backs.
Screening mammography is the only proven method to reduce deaths due to breast cancer. In the end, providers and patients need to be allowed to make an educated decision based on real science regarding the multiple benefits and the highly advertised limitations of screening mammography. It shouldn’t be a debate or rocket science, just common sense.
Screening Guideline comparison chart: http://densebreast-info.org/screeningguidelines.aspx